
Generic Run Report free printable template
Show details
GENERIC RUN REPORT Prehospital Patient Care Chart INCIDENT NUMBER INCIDENT ADDRESS UNIT ID INCIDENT CITY INCIDENT DATE INCIDENT ZIP CODE INCIDENT LOCATION TYPE See Ref. Sheet COMPLAINT REPORTED BY DISPATCH See Ref. Sheet PRIMARY PAYMENT EMERGENCY MEDICAL DISPATCH PERFORMED No Yes w/pre-arrival instructions Yes w/out pre-arrival instructions LEVEL OF SERVICE BLS Emergency ALS Level 1 Emergency ALS Level 2 Specialty Care Transport Treated Transport EMS No Patient Found Helicopter Cancelled No...
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign patient care report template form
Edit your ems patient care report pdf form online
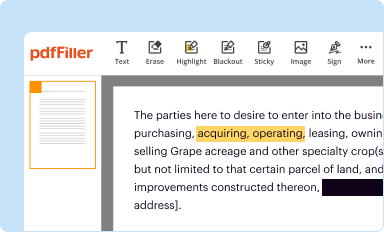
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
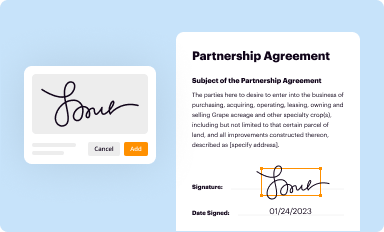
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
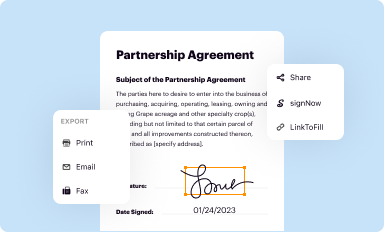
Share your form instantly
Email, fax, or share your ems report template form via URL. You can also download, print, or export forms to your preferred cloud storage service.
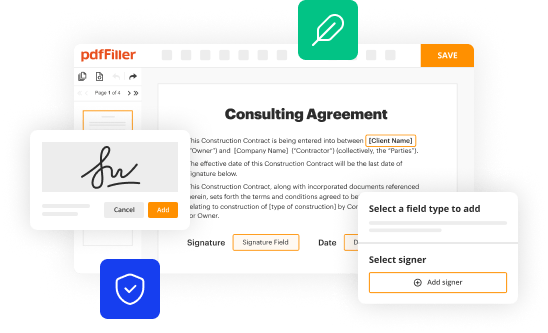
Editing patient care report online



Follow the guidelines below to use a professional PDF editor:
1
Log in to your account. Start Free Trial and sign up a profile if you don't have one.
2
Upload a document. Select Add New on your Dashboard and transfer a file into the system in one of the following ways: by uploading it from your device or importing from the cloud, web, or internal mail. Then, click Start editing.
3
Edit generic ems run report form. Replace text, adding objects, rearranging pages, and more. Then select the Documents tab to combine, divide, lock or unlock the file.
4
Save your file. Select it from your records list. Then, click the right toolbar and select one of the various exporting options: save in numerous formats, download as PDF, email, or cloud.
With pdfFiller, dealing with documents is always straightforward. Try it now!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out patient care report pdf form
How to fill out Generic Run Report
01
Open the Generic Run Report template.
02
Fill in the report header with the project title and identification details.
03
Enter the date of the report submission.
04
Provide the name and contact information of the person preparing the report.
05
List the objectives and goals of the run in the designated section.
06
Detail the methodology used during the run, including tools and processes employed.
07
Record any observations made during the run, including successes and challenges.
08
Summarize the results, including any key metrics or benchmarks achieved.
09
Include a conclusion that discusses the implications of the run results.
10
Attach any relevant appendices or supporting documents.
11
Review the completed report for accuracy and clarity before submission.
Who needs Generic Run Report?
01
Project managers who need to assess the progress of a project.
02
Team members who require a record of run outcomes.
03
Stakeholders who want to evaluate the effectiveness of processes.
04
Quality assurance teams needing to monitor compliance with standards.
05
Executives needing summary reports for decision-making.
Fill
patient care report form
: Try Risk Free
People Also Ask about patient care reports
What does chart stand for EMS?
C.H.A.R.T. C = Chief Complaint. H = History (Past & Present) A = Assessment. R = Rx or Treatment.
How do you write a patient care report?
What Patient Care Reports Should Include Presenting medical condition and narrative. Past medical history. Current medications. Clinical signs and mechanism of injury. Presumptive diagnosis and treatments administered. Patient demographics. Dates and time stamps. Signatures of EMS personnel and patient.
What does the R in chart stand for?
An X-bar and R (range) chart is a pair of control charts used with processes that have a subgroup size of two or more. The standard chart for variables data, X-bar and R charts help determine if a process is stable and predictable.
What is the acronym for chart?
Community Health Access and Rural Transformation (CHART) Model Fact Sheet.
What is a chart narrative?
What is Narrative Chart? Narrative Chart is an open-source visualization library specialized for authoring charts that facilitate data storytelling with a high-level action-oriented declarative grammar. It enables users to rapidly create expressive charts and inspires creativity.
What do you document in a patient chart?
As such, the chart should include all pertinent details from a nurse's contact with the patient. This includes all care provided, including patient education and relevant family interactions. Everything should be documented to medical necessity in order to provide a thorough record of care.
Our user reviews speak for themselves
Read more or give pdfFiller a try to experience the benefits for yourself
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I modify chart patient care report without leaving Google Drive?
Using pdfFiller with Google Docs allows you to create, amend, and sign documents straight from your Google Drive. The add-on turns your generic ambulance run report into a dynamic fillable form that you can manage and eSign from anywhere.
How can I get pcr template ems?
With pdfFiller, an all-in-one online tool for professional document management, it's easy to fill out documents. Over 25 million fillable forms are available on our website, and you can find the prehospital care report in a matter of seconds. Open it right away and start making it your own with help from advanced editing tools.
Can I create an electronic signature for signing my ambulance patient care report form in Gmail?
Create your eSignature using pdfFiller and then eSign your blank ems patient care report template immediately from your email with pdfFiller's Gmail add-on. To keep your signatures and signed papers, you must create an account.
What is Generic Run Report?
A Generic Run Report is a standardized document used to summarize the results of a specific process or operation within a certain time frame. It compiles various performance metrics and data that allow organizations to evaluate efficiency and outcomes.
Who is required to file Generic Run Report?
Individuals or departments responsible for overseeing and managing specific operations or projects are typically required to file a Generic Run Report. This can include managers, operations staff, or compliance officers.
How to fill out Generic Run Report?
To fill out a Generic Run Report, you should gather all relevant data regarding the operation or process being reviewed, such as performance metrics, time logs, and any irregularities. Then, follow the specified format and guidelines to record this information accurately, ensuring that all required sections are completed.
What is the purpose of Generic Run Report?
The purpose of a Generic Run Report is to provide a clear and concise overview of the performance of certain processes, highlight areas for improvement, track progress over time, and ensure compliance with regulatory or internal standards.
What information must be reported on Generic Run Report?
Information that must be reported on a Generic Run Report includes date and time of operation, key performance indicators, operational efficiencies, any disruptions or issues encountered, corrective actions taken, and overall conclusions regarding the performance of the operation.
Fill out your Generic Run Report online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Ems Patient Care Report is not the form you're looking for?Search for another form here.
Keywords relevant to emt chart example
Related to ems run sheet




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
